MD3T™ Multi-Directional Tibial Tubercle Transfer System
For Medial, AMZ, Anterior, Distal, and Proximal Transfers.
![]()
Before Transfer
![]()
After Transfer
System Designed By:
Alan C. Merchant, MD
Clinical Professor, Emeritus, Stanford
Staff Surgeon, Emeritus, El Camino Hospital
Mountain View, CA
Flexible and Simple.
A simple set of instruments allows for precise creation of two compound wedges of bone. Transposing these wedges medializes the tubercle.



“The MD3T system allows for precise and reproducible correction of tibial tuberosity position in all three planes. This versatility makes it my ‘go-to’ for unloading patellofemoral chondrosis and/or correcting aberrant force vectors in the setting of instability. Additional benefits of the MD3T include less invasive soft tissue dissection and maintenance of the lateral tibial cortex creating a smaller cortical defect, which help reduce pain and improve construct stability for earlier weight-bearing and range of motion.”
Seth L. Sherman, M.D., Stanford HealthCare
“Because of the surgical benefits of the MD3T procedure relative to the AMZ, I have no doubt that this approach will ultimately become the new world standard. The MD3T system will allow the average orthopedic surgeon to safely and reproducibly perform a tubercle transfer.”
Scott F. Dye, M.D., University of California at San Francisco
The MD3T Story…
Transferring the tibial tubercle (TT) to treat patellofemoral disorders is a time-tested and well-established surgical technique. Medial transfer has been practiced since 18881, and anterior transfer was introduced by Maquet in 19762. In 1983, Fulkerson combined these two transfers in the antero-medialization (AMZ) technique3. In addition, distal transfer to correct patella alta, and lateral transfer to reconstruct an over-medialized TT, are occasionally indicated. The Multi-Directional Tibial Tubercle Transfer (MD3T) System from Kinamed has unique advantages: it enables the surgeon to move the TT in multiple directions in a precise, predictable, and independent manner, while preserving greater cortical integrity to help reduce the risk of a tibial stress fracture. The concept of the MD3T Technique4,5 is simple:
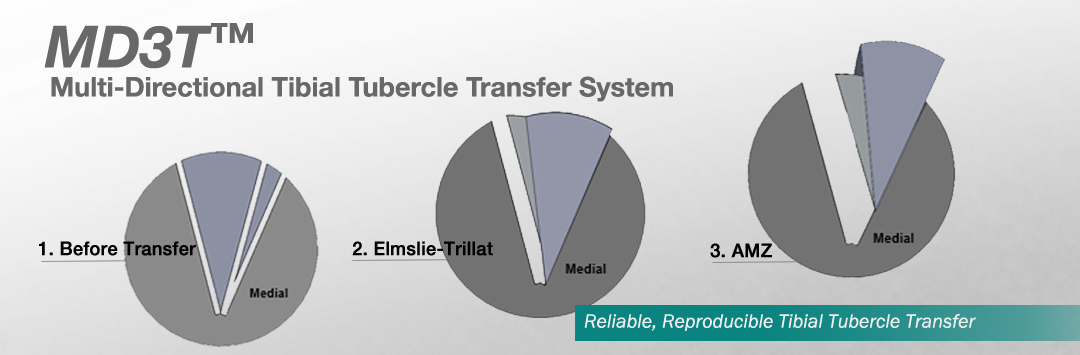
• A compound wedge of bone containing the Tibial Tubercle and its attached Patellar Tendon is created, the “Primary Wedge.”
• For corrections that include medialization, a “Secondary Wedge” of bone is created medial to the Primary Wedge.
• The Primary and Secondary Wedges are transposed, thus transferring the Tibial Tubercle medially. The width of the Secondary Wedge determines the medial transfer distance.
• For medial transfer, fast-setting bone void filler or bone graft is used to fill the space lateral to the transposed Wedges prior to fixation.
• For antero-medial transfer, additional fast-setting bone void filler or bone graft is placed lateral and posterior to the transposed Wedges prior to fixation.
• The medial and anterior transfer distances can therefore be planned independently of one another.
• Unidirectional anterior, distal, and proximal transfers involve the repositioning of the Primary Wedge only (a Secondary Wedge is not created).
1. Roux (1888) Luxation Habituelle de la Rotule. Rev Chir Paris. 8:682-689.
2. Maquet (1976) Advancement of the tibial tuberosity. Clin Orthop. 115:225-230.
3. Fulkerson (1983). Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop.
177:176–181.
4. Merchant (2001) Patellofemoral Joint Disorders. In: Chapman’s Orthopedic Surgery, 3rd ed, pp. 2334-2335, edited by M.W. Chapman. Lippincott Williams & Wilkins, Philadelphia.
5. Merchant et al (2016) Multi-Directional Tibial Tubercle Transfer Technique: Rationale and Biomechanical
Investigation. Journal of Surgical Orthopedic Advances. 25(3):157-164.
Patents
U.S. Patents 7,794,466 and 8,828,010. Additional U.S. and International Patents Pending